Consents ipad

- I understand that buprenorphine/naloxonecombination or buprenorphine mono-productis an opiate and has the same addictiveproperties as other opiates, such as heroin, methadone, codeine, morphine and OxyContin. Stopping buprenorphine/naloxone combination or buprenorphine mono-product suddenly will result in the same withdrawal symptoms and put me at the same risk ofrelapse as with other opiates.
- I agree to keep and be on time to all myscheduled appointments with the doctor. If I am delayed or I must reschedule my appointment, I will notify the office in atimely way.
- I agree to conduct myself in a courteousmanner towards all staff and other patients.
- I agree to provide urine for the purposeof toxicology screens at any time duringmy treatment.
- I agree to participate in group therapy at the time of my appointment.
- I agree not to arrive at the office intoxicated or under the influence of drugs.If I do, I will not be given medication until my next scheduled appointment.
- I agree that my medication prescription can be given to me only at my office visits and only by the doctor. If I miss scheduled office visits, I may not be able toget a Suboxone prescription until the next scheduled visit.
- I agree to take my medication as the doctor has instructed and not to alter the way I take my medication without first consulting the doctor.
- I agree that the medication I receive ismy responsibility and that I will keep itin a safe, secure place, away from children, pets or any person who could potentially abuse it. I understand that lost medication will not be replaced.
- I agree not to sell, share, or give any of my medication to another individual. Iunderstand that such mishandling of my medication is a serious violation of this agreement and would result in my treatmentbeing terminated.
- I agree not to obtain any medications from any physicians, pharmacies, or other sources without informing my treating physician. I understand that mixing buprenorphine/naloxone combination or buprenorphinemono-product with other medications, especially benzodiazepines (Xanax, Ativan, Valium, Klonopin), alcohol or other drugsof abuse, can be dangerous. I also understand that a number of deaths have been reported among individuals mixing buprenorphine/naloxone combination or buprenorphine mono-product with benzodiazepines.
- I understand that medication alone is notsufficient treatment for my addiction, a
n d I a g r e e t o p a r t i c i p a t e i n c r e a t i n g a n d carrying out a recovery treatment plan.This plan will be revised, with my inputand as needed, to assist me in my recovery. - If I decide to stop buprenorphine/naloxone combination or buprenorphine mono-product therapy at any time, I will work withthe treatment nurse and doctor to taper slowly (to reduce discomfort and relapse potential) or to transfer to a methadone program.

This release of information is intended to provide coordination of care between SpecialistsMAT, PSC and . You are givng SpecialistsMAT, PSC and the authority to share medical records and to speak with each other for the purpose of coordination of medical care and the treatment plan.
I authorize the SpecialistsMAT, PSC and to share or disclose all of my medical records, including any specially protected records, such as those relating to psychological or psychiatric impairments, substance use disorders, and medical or surgical treatments.
I authorize SpecialistsMAT, PSC and to coordinate care with professionals and health care delivery systems as clinically appropriate. Coordination of care may include treatment updates, psychotherapy notes, and laboratory findings.
If you do not want certain portions of your medical records released, please read this section carefully and identify the information you do not want released. Otherwise, your records will be released as specified above.
I understand that I may revoke the authorization at any time prior to the expiration date or event, but that my revocation will not have any effect on actions taken by SpecialistsMAT, PSC or its physicians, employees or agents before they received my revocation. Should I desire to revoke this authorization, I must send written notice to SpecialistsMAT, PSC.
I understand that I am not required to sign this authorization. SpecialistsMAT, pSC or its physicians, employees will not condition treatment, payment, enrollment or eligibility for benefits on whether I provide this Authorization.
I understand that my records may be subject to disclosure by the recipient and may no longer be protected by federal privacy regulations. I understand that this Authorization does not limit SpecialistsMAT, PSC or its physicians, employees its physicians’, employees’ or agents’ ability to use or disclose my information for treatment, payment, or health care operations, or as otherwise permitted by law.
This release of information expires in 1 year after signature date.
- We will ensure that your pain treatmentswill be as safe as possible.
- We will monitor your prescriptions and test for substance abuse to ensure you aretaking your medications safely and correctly.
- We will recommend other forms of treatment, such as physical therapy, behavioral therapy, addiction counseling, and injection therapy, to help you with your pain condition and improve functioning.
- We will set treatment goals and monitor your progress in achieving those goals.
- When there is imminent danger to the patient or another person.Under circumstances of suspected child, elder, or dependent adult abuse or neglect.
- When disclosure must be made to medical professionals in the case of a medical emergency.
- When the mental health professional is compelled by law to disclose client records.

I authorize SpecialistsMAT to disclose to the State and/or local Department of Health officials that require the following reports:
(1) Information that State law requires to be reported about my diagnosis and treatment for: HIV infection, AIDS, STD (sexually transmitted disease), and TB (tuberculosis)
(2) My name and other personal identifying information, if required to be reported by State law;
(3) Information about my status as a patient in alcohol or drug treatment, if required to be reported by State law.
The purpose of the disclosure authorized herein is to allow my alcohol or drug treatment program to comply with State law(s) requiring the reporting of cases of HIV/AIDS/STD/TB.
I understand that my records are protected under the Federal regulations governing Confidentiality of Alcohol and Drug Abuse Patient Records, 42 C.F.R. Part 2, and cannot be disclosed without my written consent unless otherwise provided for in the regulations. I also understand that HIV-related information about me, STD-related information about me, and TB related information about me is protected byState law and cannot be disclosed unless the disclosure is authorized by State law. I also understand that I may revoke this consent at any time except to the extent that action has been taken in reliance on it, and that in any event this consent expires automatically 1 year from the date of this consent.



URINE TOXICOLOGY SCREENING POLICY
1) All belongings (coats, bags, etc.) are left outside the bathroom door.
2) No washing hands until the urine sample is handed to the medical assistant.
3) No flushing of the toilet until urine sample is handed to the medical assistant.
4) Urine samples will be required at each visit.
5) Any questionable urine sample is an automatic repeat the same day.
6) Observed urines are discouraged but may be necessary. Oral swabs may be utilized in place of observed urines.
7) Tampering of urine samples may be grounds for discharge and referral to a higher level of care.

Prior Authorization
I give permission to SpecialistsMAT, PSC to submit authorization requests on my behalf, and if necessary, to appeal the denial of any ordered medications.

TELEMEDICINE CONSENT
Telemedicine services is the practice of health care delivery, diagnosis, consultation, treatment, transfer of medical data, and education using interactive audio, video, or data communications. I understand that telemedicine also involves the communication of my medical/mental information, both orally and visually, to health care practitioners. I agree to participate in a telemedicine evaluation/supervision. By signing this agreement, I authorize the electronic transmission of my medical information and/or videoconference session so that it can be viewed by a doctor and other persons involved in my medical or mental health care. I understand that as with any technology, telemedicine does have its limitations. There is no guarantee, therefore, that this telemedicine session will eliminate the need for me to see a specialist in person. I understand there are potential risks with this technology: (1) The video connection may not work or that it may stop working during the consultation. (2) The video picture or information transmitted may not be clear enough to be useful for the consultation. (3) I may be required to go to the location of the consulting physician if it is felt that the information obtained via telemedicine was not sufficient to make a diagnosis. I give my consent to be interviewed by the consulting health care provider. I also understand other individuals may be present to operate the video equipment and that they will take reasonable steps to maintain confidentiality of the information obtained. I authorize the release of any relevant medical information about me to the consulting health care provider, any staff the consulting healthcare provider supervises, third party payers and other health care providers who may need this information for continuing care purposes. Upon completion of virtual services, I authorize SpecialistsMAT, PSC representatives, to sign on behalf of the responsible adult where a responsible adult/parent/caregiver signature is required for insurance or other payor documentation. I hereby release SpecialistsMAT, PSC, its personnel and any other person participating in my care from any and all liability which may arise from the taking and authorized use of such videotapes, digital recording films and photographs. I have read this document and understand the risk and benefits of the telemedicine consultation and have had my questions regarding the procedure explained and I hereby consent to participate in a telemedicine visit under the conditions described in this document.

In order to provide you with the best possible care, SpecialistsMAT utilizes text messaging and email to facilitate communication and engagement with its patients. Text messages and emails may include appointment reminders, general inquiries regarding appointments and medications, and in office messaging to provide you with an efficient appointment experience. Text messaging and email are not secure forms of communication, but they are HIPAA compliant through the avoidance of individually identifiable health information in the transmitted messages. I understand that message/ data rates may apply to messages sent under my cell phone plan. For additional details regarding this policy, please direct your questions to a staff member.


Thank you for completing your new patient paperwork.
Click on the SUBMIT BUTTON below.
Go to the Team Member at the front counter.

Dietary Requirements Template
Collect important information about food restrictions and allergies. Save submissions as PDFs. Easy to customize, download, print, and share with kitchen staff.
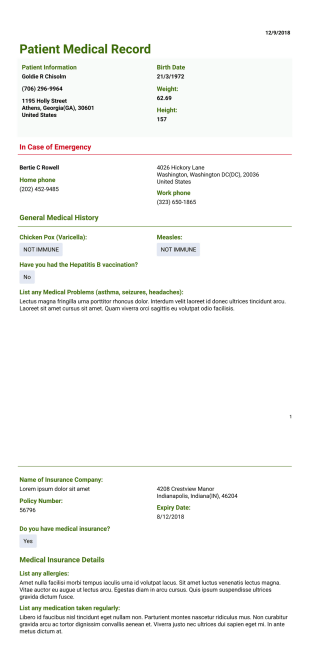
Patient Medical Record Template
Medical History Record PDF template lets you collect the patient's data such as personal information, contact information in an emergency case, general medical history. By using this sample, the doctor ensures the patient's better care and treatment.
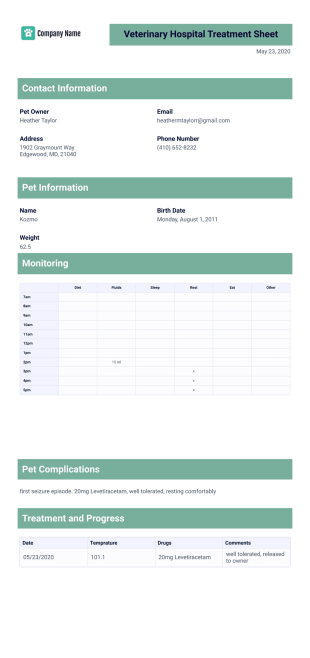
Veterinary Hospital Treatment Sheet Template
Veterinary Hospital Treatment Sheet helps both the hospital and pet owners in understanding and tracking a pet's treatment process. Just like any other hospitals, keeping patient's treatment records is necessary to monitor progress and make sure proper treatment is given. Having a veterinary treatment sheet also helps in planning and evaluating other treatments for the pet, facilitating research and creating a record for the pet's future care. If you are trying to create a treatment sheet and looking for a sample template, then look no further because Jotform offers a Veterinary Hospital Treatment Sheet template you can download, save, edit and print. This Veterinary Treatment Sheet template contains the necessary information for recording and tracking treatment process for your client's pet. It has information such as name of client, date and time, address, contact number, treatment performed, doctor's name, monitoring progress report and many more. This template is editable and allows you to add more information or remove if you need to. Add your hospital's logo or insert images to make it more personalized.

Child Medical History Template
This child medical history PDF template makes checking patients vitals and recording that important data easy. Add your own branding, adjust fields for your specific needs and then simply print out your PDF for the patient's file.

Dental Health Record Template
The Dental Health Record Template is easy for patients to fill out and designed to get the doctor the most important information. Patients can fill out their information on a computer or tablet using our Dental Health Record Template.

Medical Case Report
Provide the best health care to the people by using evidence-based care study by using this Medical Case Report template. This template contains all the information required in conducting research and report.
These templates are suggested forms only. If you're using a form as a contract, or to gather personal (or personal health) info, or for some other purpose with legal implications, we recommend that you do your homework to ensure you are complying with applicable laws and that you consult an attorney before relying on any particular form.