Boy Scout Camp Physical Form
A Boy Scout Camp Physical Form is a health information form that is compliant to the standards of the Boy Scouts of America. This is a necessary document for any camping activity longer than three consecutive days. This form acts as a multi-purpose form by promoting health awareness. It also serves as an information reference for health officials who may give the person treatment in case of illness or injury during the camping trip. This also serves as the participant's physical preparedness for specialized activities like a jamboree.
This Boy Scout Camp Physical Form PDF template is your quick and comprehensive form for both the applicant and the physician. With the use of the web form, participants or applicants can fill the form and submit it online. No need to fill out paper documents and have better filing management with a database on the cloud. Have a copy of this Jotform based Boy Scout Camp Physical Form PDF Template and start receiving physical fitness forms for your boy scout activities!
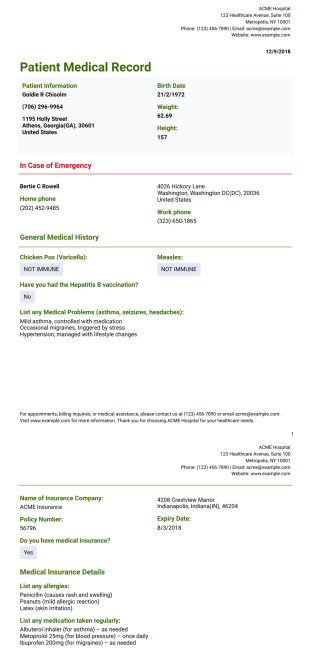
Patient Medical Record Template
Medical History Record PDF template lets you collect the patient's data such as personal information, contact information in an emergency case, general medical history. By using this sample, the doctor ensures the patient's better care and treatment.

Patient Medical History Template
Through Medical History Record PDF template, patients provide their personal information needed to see the doctor. Thanks to this medical history record sample, the doctor knows about patients medical history.

First Aid Incident Report Template
Incidents must be reported and recorded to be sure that correct actions and treatment are made which should trigger management awareness and an investigation. The First-Aid Incident Report template contains injured person's personal details and contact details, the details and visible symptoms of injury, the Glasgow Coma Scale which is a neurological scale that expects to give a dependable and target method for chronicle the condition of an individual's awareness and brief information of treatment. Also, it contains the profile of the first-aider and signature of the person who prepares the report.

Child Medical History Template
This child medical history PDF template makes checking patients vitals and recording that important data easy. Add your own branding, adjust fields for your specific needs and then simply print out your PDF for the patient's file.

Simple Medical History Template
Once you have collected these medical data, you can record them as a pdf by using this medical history PDF template. In addition, you don't need to be worried about the safety of data.

Short Medical History
Medical History Record PDF template is mostly used in order to provide significant information about the health history, care requirements, and risk factors of the patient to doctors. It is for collecting data from the patients.
These templates are suggested forms only. If you're using a form as a contract, or to gather personal (or personal health) info, or for some other purpose with legal implications, we recommend that you do your homework to ensure you are complying with applicable laws and that you consult an attorney before relying on any particular form.